I have built this website with the simple view of giving you Parents or Family members an idea of what you’re dealing with, I have searched the world internet looking for up to date data, with the help of many world Surgeons I talk to some have given me permission to use their videos on operations they themselves have done.
What you find here is an in-depth look of a child born unable to swallow, by now you might have seen I myself was born in 1962 in England unable to swallow, this website makes no money and is fully self-funded by me, in an attempt at putting something back, to help others like yourself. If you like this site please share with others.
This is the page for Mothers Who are having babies born unable to Swallow
A Video from Parents of a child born with Ea-Tef who at one point thought the worse, please watch and read, before you go down this page
Baby’s born unable to Swallow
I can relate to what I am about to talk about regarding this Small Family unit, having been in their shoes years before with my own daughter, who was one of 100 known cases in the world, and Doctors who struggled to grasp what they were dealing with.
I came across this Family doing what I do in a group and via this website, but we are going back a few years, and the site was in it’s younger years. Mum and I started talking, she was very scared that her child would not make it because the Doctors looking after her child seemed overwhelming. Long story cut short, I was able to ask two other world surgeons to step in and help the team looking after their child, allowing all concerned too, in a word teach and nurture the team looking after their child.
There have been some real low points on this trip of 112 days spent in the hospital, but without the help from others in other parts of the world may be the outcome would sadly have been different. Sometimes believing in others and working as a team things can change, so never give up, at first you might feel like your world has fallen apart but trust me, you won’t be alone, we are here for you.
I asked the Parents if I could run this video on this page for New Parents to see there is light at the end of their tunnel.
Stats as we found them
Esophageal atresia is the most common GI atresia. The estimated incidence is 1 in 3500 live births. Other congenital malformations are present in up to 50% of cases.
Two syndromes, in particular, are associated with esophageal atresia:
VACTERL (vertebral anomalies, anal atresia, cardiac malformations, tracheoesophageal fistula, esophageal atresia, renal anomalies, and radial aplasia, and limb anomalies)
CHARGE (coloboma, heart defects, atresia of the choanae, retardation of mental and/or physical development, genital hypoplasia, and ear abnormalities)
About 19% of infants with esophageal atresia meet the criteria for VACTERL.
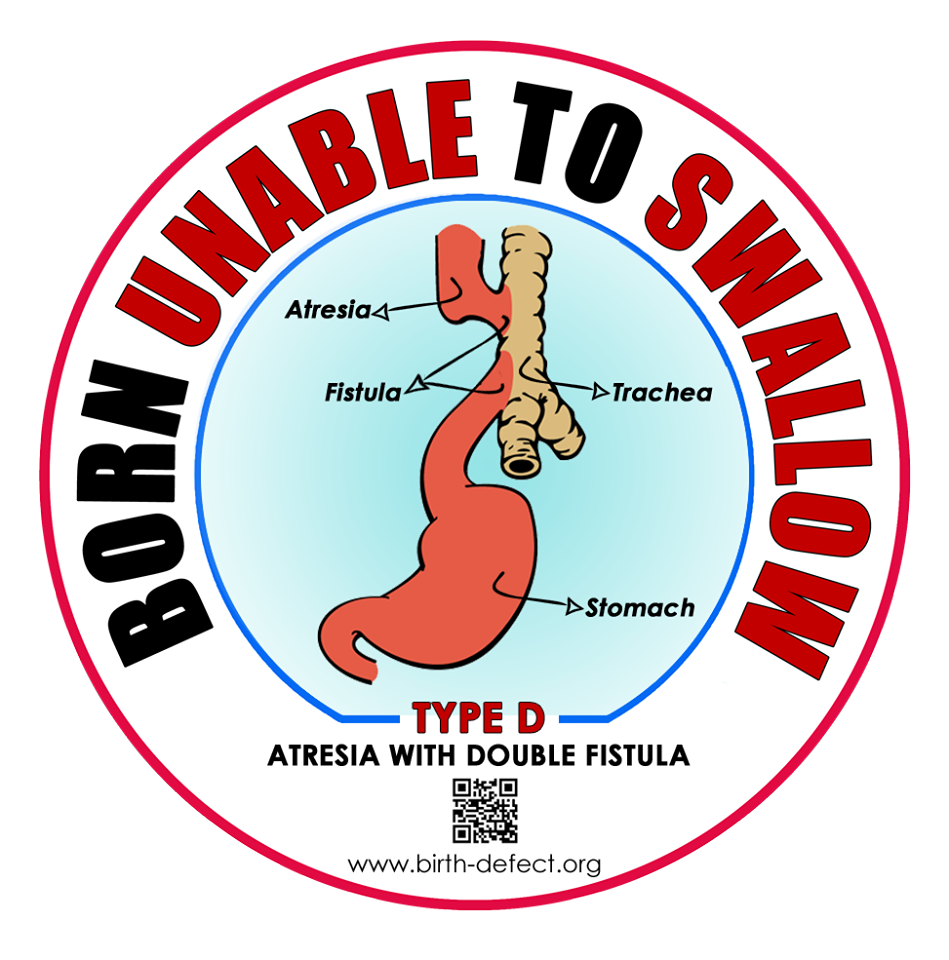
There are 5 major types of esophageal atresia. Most of the types also involve a fistula between the trachea and the esophagus. (photos found lower down the page)
Most infants present during the neonatal period, but infants with the H type fistula may not present until later in life.
Characteristic signs are excessive secretions, coughing and cyanosis after attempts at feeding, and aspiration pneumonia. Esophageal atresia with a distal fistula leads to abdominal distention because, as the infant cries, air from the trachea is forced through the fistula into the lower esophagus and stomach.
Tracheo-Oesophageal Fistula (TOF) and Oesophageal Atresia (OA) are rare congenital conditions of the esophagus (food pipe) and/or trachea (airway) that affect one in every 3,500 babies. But is becoming more common these days according to recent research. Babies born with TOF or TEF need to have intensive neo-natal care prior to corrective surgery, normally within days of birth.
Some children have to undergo additional surgical interventions later on in their lives. Whilst many children born with TOF or TEF will experience only a few problems, others may have difficulties with swallowing and digesting food, Gastro-Oesophageal Reflux (where the acidic stomach contents pass back into the lower esophagus) and respiratory problems. The effects of surgery and associated health problems can add a great deal to the usual challenges of parenthood. All this above is explained in detail on this website.
Currently, nobody knows what causes TOF-OA or EA-TEF. For the new parent of a TOF or TEF child, this is very important to understand – it was not your fault, you couldn’t have done anything to prevent it, as your read with-in this website.
With the benefits of modern medical intervention and the active support of groups, the outlook for children with TOF-OA & EA-TEF is very positive.
OA or EA
In Oesophageal Atresia (OA) (UK) way of wording, EA is the way of other countries, the baby is born with a pouch at the top of its esophagus (food pipe) which prevents food from reaching the stomach. Prior to surgery, this pouch can fill up with food and saliva, which can eventually overflow into the baby’s trachea (windpipe), entering the lungs and causing choking.
TOF or TEF
In Tracheo-Oesophageal Fistula (TOF), the bottom end of the baby’s esophagus is joined to its trachea (windpipe). Without surgical intervention, this causes air to pass from the windpipe to the food pipe and stomach. It can also allow stomach acid to pass into the lungs. Again on this website, you can view x-ray photos and even 3D video to help you understand better.
Birth Mum is found to have Polyhydramnios What is this?
What is polyhydramnios?
This is very interesting it will size up so you can hear and see.
Polyhydramnios vs. Oligohydramnios
Polyhydramnios means you have too much amniotic fluid in your womb (uterus). It happens in fewer than one in 500 pregnancies in the UK, so it isn’t common. Most cases of polyhydramnios are mild or moderate.
The amniotic fluid surrounding your baby protects him from being hurt if you have a blow your tummy or if your tummy is squashed.
The fluid also protects your baby against infection, as well as helping his lungs to develop. The amount of fluid around your baby gradually increases until there is about one liter (1.8 pints) surrounding him at 37 weeks. This amount usually decreases to around half a liter (0.9 pints) by 40 weeks Your baby will regularly swallow amniotic fluid, which then passes out of his body as urine. This is how he controls the volume of amniotic fluid around him. When this delicate balance is disturbed, the volume of amniotic fluid can increase rapidly.
Polyhydramnios is usually diagnosed when the amniotic fluid volume reaches two liters (3.5 pints) or more. In severe cases of polyhydramnios, there may be as much as three liters (5.3 pints) of fluid, or three times the normal amount, around your baby.
How can I tell if I have polyhydramnios?
It can sometimes be hard for you to tell since your body is continually changing throughout pregnancy. However, you may notice that your tummy is getting unusually large and feeling more taut than usual and that your skin is stretched and shiny. You may feel uncomfortable and breathless and find it hard to climb a flight of stairs.
Polyhydramnios tends to build up gradually, so it is often picked up from about 30 weeks of pregnancy when the levels of fluid have got noticeably higher. However, in rare cases, it can come on very rapidly over the course of just a few days so maybe picked up earlier in pregnancy or during the mid-pregnancy scan Rapid, acute polyhydramnios is more common if you’re having twins or more.
Imaging of Congenital Anomalies of the Gastrointestinal Tract
Department of Radiodiagnosis, All India Institute of Medical Sciences, New Delhi, India. (To give you just an idea as to how things work)The radiological imaging plays a vital role in the evaluation of patients with congenital anomalies of the gastrointestinal tract. The evaluation of these patients, most of which present early after birth, frequently requires the use of various imaging modalities for making the correct diagnosis and planning surgical correction.
This article reviews the common congenital anomalies of the gastrointestinal tract including obstructive lesions, anomalies of rotation and fixation, anorectal anomalies, and intestinal duplications. The plain radiograph is often diagnostic in neonates with complete gastric of upper intestinal obstruction and further radiologic evaluation may be unnecessary.
An upper gastrointestinal series should be performed in all patients with incomplete intestinal obstruction. Sonography is useful in the evaluation of many congenital anomalies affecting the pediatric gastrointestinal tract especially hypertrophic pyloric stenosis, enteric duplication cysts, midgut malrotation, meconium ileus, and meconium peritonitis.
This video is around 43 mins long, this is very interesting giving out much info, the lady talking is from Boston USA, if you have a spare 43 mins then you will find this talk very interesting like l did much info given.
Moreover, CT and MRI have assumed greater importance as these provide excellent anatomic details which may be necessary for correct diagnosis as well as treatment planning. This is particularly true for the evaluation of congenital anomalies such as esophageal/enteric duplications, vascular rings, and anorectal anomalies.
It is important to be familiar with the role and usefulness of the various imaging modalities so that these can be used judiciously to avoid unnecessary radiation exposure while minimizing the patient discomfort. A wide spectrum of congenital anomalies may affect the gastrointestinal tract, some of which manifest early after birth while others may not present till late childhood or adulthood.
Imaging plays a very useful role in these developmental lesions, most of which present with obstruction. In most cases, plain radiography, gastrointestinal contrast study or Ultrasound (US) suffice. Computed tomography (CT) and Magnetic Resonance Imaging (MRI) are increasingly proving more useful to provide an accurate diagnosis, especially in difficult cases. Developmental lesions of the neonatal gastrointestinal tract can be grouped as follows: Structural Attributed to embryologic maldevelopment Oesophagal atresia with or without fistula.
An amnioreduction is the repeated removal of a large volume of amniotic fluid (bag of waters) via a procedure called amniocentesis or amniotic fluid testing. The procedure aims to normalize excessive fluid levels caused by a condition called polyhydramnios. It relieves discomfort in the mother, improves blood flow from the placenta to the uterus (particularly in the setting of twin to twin transfusion syndrome/TTTS), and prevent premature delivery.
Too much water in the bag that surrounds the baby in the uterus exerts pressure on the mother and baby, causing difficulty breathing in the mother, premature delivery in the fetus, and several other complications. Excessive amniotic fluid is also produced in the recipient twin in TTTS and exerts pressure on the donor twin, interfering with its growth. Amnioreduction serves to enhance blood flow to the donor twin by lowering pressure inside the bag of waters.
The doctors avoid amnioreduction in the presence of the following factors:
Bleeding disorder in the mother or fetus
Premature uterine contractions and labor
Suspected infection of the coverings of the developing fetus (chorioamnionitis)
An amnioreduction is performed under ultrasound guidance. A sterile needle is advanced into the amniotic fluid through the mother’s abdomen and the fluid drained. Vacuum tubes and vacuum bottles may be used to assist drainage. Fetal well-being is monitored by non-stress testing at the same time. The goal is to reduce pressure on the surface of the placenta and to limit the mother’s discomfort.
Do I need amnioreduction to treat my polyhydramnios?
One way to treat polyhydramnios is by directly draining amniotic fluid from the uterus. This procedure, called amnioreduction, is similar to amniocentesis for genetic testing. Because amnioreduction does not resolve problems that may underlie polyhydramnios, it may need to be repeated during your pregnancy. Amnioreduction comes with a small risk of complications, such as cramping, bleeding, and, more rarely, miscarriage. If your polyhydramnios does not seem to be causing complications for you or the fetus, your doctor may recommend oral medication or no treatment at all.
It depends on the unique circumstance of each pregnancy. Amnio-reduction is an invasive procedure with risk to both the mother and fetus. In addition, depending on the cause of the polyhydramnios, the excessive volume of fluid may re-accumulate after the amnio-reduction. However, amnio-reduction may be beneficial in gaining time for fetal maturation or reducing maternal symptoms. The decision needs to be made collaboratively between the woman and the health-care team.
Women undergoing the procedure are at risk of premature rupture of membranes, premature separation of the placenta, and chorioamnionitis.
After birth How do I know if my Baby has a swallowing problem?
Normally, individuals rarely choke during a meal. Occasionally, food will stick in the oesophagus for a few seconds (especially solid foods) but will pass spontaneously or can be washed down easily with liquids. However, there are a number of symptoms that require evaluation for a possible swallowing problem, including:
Frequent choking on food.
Hesitancy in food passage for more than a few seconds.
Pain when swallowing.
Recurring pneumonia (an indication that food may be going into the lungs rather than the oesophagus).
Urgent evaluation by a doctor is required when food becomes lodged in the oesophagus for more than 15 minutes and will not pass spontaneously or with liquids. Some people are unaware that they have swallowing problems because they compensate unconsciously by choosing foods that are easier to eat, or they eat more slowly. They are at risk of choking or having large pieces of solid food lodge in the oesophagus if they let down their guard.
How are swallowing problems diagnosed?
If you feel you have a swallowing problem, your doctor will decide which phase of swallowing needs to be tested. She will order the appropriate tests after asking questions to determine the details of your swallowing symptoms and previous medical problems, as well as performing an appropriate physical examination. Three tests are most commonly used to evaluate a swallowing problem:
Barium swallow and follow through. The patient swallows a barium preparation (liquid or other forms that show up under X-ray) and an X-ray machine with video recording capability is used to view its movement through the oesophagus. This is often performed under the guidance of a speech and language therapist, an expert in swallowing as well as speech.
Upper endoscopy A flexible, narrow tube (endoscope) is passed into the oesophagus and projects images of the inside of the pharynx and oesophagus on a screen for evaluation.
Manometry This test measures the timing and strength of oesophageal contractions and muscular valve relaxation.
Among other tests that may be necessary, according to the specific needs of the individual, are an impedance test and a pH probe test (for acid reflux) this is talked about on a different page of this site.
How are swallowing problems treated?
The form of treatment for your swallowing problem will depend on the type of problem a person has. Sometimes, the problem will resolve itself without treatment. On other occasions, the condition can be managed easily, such as by using a special tool called an esophageal dilator to stretch an oesophagus narrowed from acid reflux. However, the problem may be complex, requiring a specialist or the coordination of several specialists. If you have a chewing or swallowing problem there are several things you can do to make eating and drinking easier and safer, including:
Positioning
Sit upright at a 90-degree angle.
Tilt your head slightly forward.
Remain sitting upright or standing for 15 to 20 minutes after eating a meal.
Dining environment
Minimize distractions in the area where you eat.
Stay focused on the tasks of eating and drinking.
Do not talk with food in your mouth
Amount and rate
Eat slowly.
Cut your food into small pieces and chew it thoroughly.
Do not try to eat more than 1/2 teaspoon of your food at a time.
Swallowing
You may need to swallow two or three times per bite or sip.
If food or liquid catches in your throat, cough gently or clear your throat, and swallow again before taking a breath. Repeat if necessary.
Concentrate on swallowing frequently.
Saliva management
Drink plenty of fluids.
Periodically suck on lollies, ice cubes or lemon ice, or drink lemon-flavored water to increase saliva production, which will increase swallowing frequency.
Food consistency
Minimize or eliminate foods that require chewing and eat more soft foods.
Purée your food in a blender.
If thin liquids cause you to cough, thicken them with a liquid thickener (your speech and language therapist can recommend one for you). You can also substitute thicker liquids for thin ones, such as syrup for juice and cream soup for plain broth.
Taking medications
Ask your pharmacist for his or her recommendations on which tablets can and should not be crushed and which medications can be prescribed in a liquid form.
Balloon Endoscopy with the CRE™ Balloon Dilator
This animation and short videoclip show’s how balloon endoscopy with the CRE™ Balloon is used to dilate strictures of the GI tract.
Look on Steven Rothernburg page on this site regarding a repair of a 3” gap by a Surgeon in the USA, Child was home in less than 3 weeks.
Barium Swallow Finds Oesophageal Atresia
Tracheoesophageal Fistula in a Newborn, seen by swallowing a Barium Meal.
A tracheoesophageal fistula was identified in the infant and surgically corrected.
Esophageal atresia (EA) – (OA) is a rare birth defect in which a baby is born without part of their esophagus (the tube that connects the mouth to the stomach). Boston Children’s Hospital’s Esophageal Atresia Treatment Program is one of the only programs in the country specifically designed to care for children with this condition
Long-Segment Colonic Interposition for Esophageal Atresia: 3D Animation (How long gap is mended on a Baby but in a 3D film) Very interesting.
Specialist Milk
The common feeding issues that babies encounter include colic, reflux, and regurgitation. The Department of Health recommends exclusive breastfeeding for the first six months.
If breastfeeding is not possible, a range of specialist kinds of milk is available to help alleviate the distress caused to babies who experience these feeding issues. Pharmacists have an important role to play in explaining what may cause different feeding issues and how they can be resolved.
Colic is one of the most common gastrointestinal complaints in babies and can affect up to one in five infants1. It can start within weeks of birth and may continue up to four-six months of age.
Virtually all infants will experience some symptoms of gastroesophageal reflux (GOR) but it is normally nothing to worry about. GOR is the effortless passage of gastric contents into the esophagus with or without regurgitation or vomiting. Symptoms peak at 3 months of age 9and usually resolve between 12 and 14 months of age.
Congenital anomalies of the esophagus comprise a diverse group of malformations. This chapter discusses embryology of the developing esophagus and esophageal anomalies secondary to its aberrant development.
The chapter also reviews major esophageal malformations as follows:
Esophageal atresia and tracheoesophageal fistula
Laryngotracheoesophageal cleft
Esophageal stenosis and webs
Foregut duplications
Congenital bronchopulmonary foregut malformations
Diverticulum of esophagus
Congenital short esophagus
The embryonic period extends from conception to the ninth week of gestation. During the latter half of the third week of development, the primitive foregut develops a ventral diverticulum that is cranial to the hepatic primordium and caudal to the fourth and fifth pharyngeal pouches. The diverticulum grows caudally and develops bronchopulmonary buds soon after the appearance. The trachea develops from a further caudal growth of the respiratory diverticulum. During the fourth and fifth weeks of development, the rapidly growing heart and liver stretch the esophagus. Because of the stretching, the esophagus narrows almost to obliteration at the level of the carina. Between the sixth and eighth weeks of gestation, the epithelium becomes 2-5 cells thick and remains stratified columnar epithelium.
Read more from the website, there are a lot of pages
Tracheo oesophageal atresia and fistula A-Z for medical students. (Interesting to watch if you are a Parent I thought) then if needed you can show your Doctor or team you might be under. This powerpoint cover’s everything about tracheoesophageal fistula and atresia, you need to know as a medical student. Not intended for patients. But if you read you will get an idea if you are a Parent, I was sent this by a Surgeon it covers anatomy, embryology, types, classification and treatment of tracheo-oesophageal fistula and atresia.
No need to put sound on.
Esophageal Atresia: Etiology, Types, Pathophysiology, Clinical Features, Diagnosis, and Treatment
TEF = TOF
Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula?
Tracheoesophageal fistula is an abnormal connection in one or more places between the esophagus (the tube that leads from the throat to the stomach) and the trachea (the tube that leads from the throat to the windpipe and lungs). Normally, the esophagus and the trachea are two separate tubes that are not connected. Tracheoesophageal fistula is also known as TE fistula or simply TEF.TE fistula is a birth defect, which is an abnormality that occurs as a fetus is forming in its mother’s uterus. When a baby with a TE fistula swallows, the liquid can pass through the abnormal connection between the esophagus and the trachea. When this happens, liquid gets into the baby’s lungs. This can cause pneumonia and other problems.
What is esophageal atresia?
TEF = TOF
fistula often occurs with another birth defect known as esophageal atresia. The esophagus is a tube that leads from the throat to the stomach. With esophageal atresia, the esophagus does not form properly while the fetus is developing before birth, resulting in two segments; one part that connects to the throat, and the other part that connects to the stomach. However, the two segments do not connect to each other. Since the esophagus is in two segments, liquid that a baby swallows cannot pass normally through the esophagus and reach the stomach. Milk and other fluids cannot be digested if the esophagus does not connect to the stomach.If a TE fistula is also present, the liquid that a baby swallows can pass through the connection between the esophagus and the trachea and go into the lungs. This can cause pneumonia and other problems.
What causes tracheoesophageal fistula and esophageal atresia?
TEF = TOF
As a fetus is growing and developing in its mother’s uterus before birth, different organ systems are developing and maturing. The trachea and the esophagus begin developing as one single tube. At about four to eight weeks after conception, a wall forms between the fetus’ esophagus and trachea to separate them into two distinct tubes. If this wall does not form properly, TE fistula and/or esophageal atresia can occur.
Which babies develop tracheoesophageal fistula or esophageal atresia?
TEF = TOF
These two problems are not thought to be inherited. However, they are often seen when a baby has other birth defects, such as:
Other digestive tract problems (such as a diaphragmatic hernia, duodenal atresia, or imperforate anus)
Heart problems (such as ventricular septal defect, tetralogy of Fallot, or patent ductus arteriosus)
Kidney and urinary tract problems (such as horseshoe or polycystic kidney, absent kidney, or hypospadias)
Muscular or skeletal problems
VACTERL syndrome (which involves Vertebral, Anal, Cardiac, TE fistula, Renal, and Limb abnormalities)
Up to one-half of all babies with TE fistula or esophageal atresia have another birth defect.
What are the symptoms of TE fistula or esophageal atresia?
TEF = TOF
The symptoms of TE fistula or esophageal atresia are usually noted very soon after birth. The following are the most common symptoms of TE fistula or esophageal atresia. However, each child may experience symptoms differently. Symptoms may include the following:
Frothy, white bubbles in the mouth
Coughing or choking when feeding
Vomiting
Blue, the color of the skin, especially when the baby is feeding
Difficulty breathing
Very round, full abdomen
Other congenital malformations might be present, such as the ones mentioned in the previous section.
Symptoms of TE fistula or esophageal atresia may resemble other conditions or medical problems. Please consult your child’s doctor for a diagnosis.
What tests are usually done to diagnose the problem?
Along with a physical examination and medical history, imaging studies are usually done to evaluate whether a baby has TE fistula and/or esophageal atresia. X-rays are taken to look at the chest and abdomen.
A small tube may also be placed into the mouth or nose and then guided into the esophagus. With esophageal atresia, the tube usually cannot be inserted very far into the esophagus. The tube’s position in the esophagus can also be seen with the X-ray.
Stricture with food bolus. Frontal view from a barium swallow examination in a patient with a repaired EA shows a stricture at the anastomotic site, with a bolus of food proximal to the stricture.
What is the treatment for TEF fistula or esophageal atresia?
If your baby has TE fistula or esophageal atresia, he or she will need surgery to fix the problem. The type of surgery depends on the following:
Type of abnormality
Overall, the health of the baby and medical history
The opinion of the surgeon and other health-care providers involved in the baby’s care
Expectations for the course of the condition
Your opinion and preference
When The fistula is repaired, the connection between the esophagus and the trachea is closed in surgery. The repair of esophageal atresia depends on how close the two sections of the esophagus are to each other. Sometimes esophageal atresia requires more than one surgery. Your baby’s surgeon and other health care providers will decide when it is best to do the operations based on your baby’s condition and the type of problem.
Could my child have problems in the future?
Some children born with esophageal atresia have long-term problems.
Swallowing food or liquids may be difficult due to:
Problems with the normal movement of foods and liquids down the esophagus (peristalsis).
Scarring that can occur in the esophagus after surgery as the wounds heal, which can partially block the passage of foods.
Sometimes, a narrowed esophagus can be widened or dilated with a special procedure done while the child is under general anesthesia. In other cases, another operation may be necessary to open up the esophagus so food can pass to the stomach properly.
About one-half of children who had esophageal atresia repaired will have problems with GERD or gastrointestinal reflux disease. GERD causes acid to move up into the esophagus from the stomach. When acid moves from the stomach into the esophagus, it causes a burning or painful feeling known as heartburn. GERD can usually be treated with medications prescribed by a doctor.
Tracheoesophageal Fistula and Esophageal Atresia in the Newborn EA = OA
Baby’s born unable to Swallow
The esophagus (food pipe) and trachea (windpipe) are 2 separate tubes. The esophagus runs behind the trachea inside the chest. Both of these tubes start at the throat. The food you eat travels down the esophagus into the stomach. The air you breathe travels down the trachea into the lungs. In some babies, these tubes don’t form correctly during pregnancy. This can lead to the problems described below. Your baby might these problems.
TOF/OA = EA=TEF
Photo 1
Tracheoesophageal Fistula and Esophageal Atresia in the Newborn
Photo 2
In normal anatomy, the trachea connects to the lungs. The esophagus connects to the stomach.
Photo 3
With esophageal atresia, the esophagus doesn’t attach to the stomach. Food can’t reach the stomach.
Photo 4
With tracheoesophageal fistula, the trachea and esophagus are connected. Air can go into the stomach, and food can go into the lungs.
Baby’s born unable to Swallow
Photo 5
With this combination of fistula and atresia, air goes into the stomach and the lungs. Food can’t reach the stomach.
E is also known as H
Baby’s born unable to Swallow
Baby’s born unable to Swallow
Baby’s born unable to Swallow
E is also known as type – H
What Is Tracheoesophageal Fistula?
A tracheoesophageal fistula (TEF) = TOF is an abnormal opening between the trachea and the esophagus. During pregnancy, the baby’s trachea and esophagus start out as one tube. During the first trimester, they are supposed to separate into 2 tubes. If the wall of tissue between the trachea and esophagus doesn’t form fully, an opening between the 2 tubes remains. This is a fistula. When the baby eats, food can pass from the esophagus through the fistula into the trachea. This can cause breathing problems. Symptoms of TEF = TOF include coughing and difficulty breathing that worsen when feeding.
Esophageal atresia is an abnormality, or birth defect, of the esophagus that occurs early in pregnancy, as the baby is developing. The esophagus forms in the first few months of fetal life as a long, hollow, continuous tube joining the mouth to the stomach. In newborns with this birth defect, the formation of this continuous esophageal tube is interrupted.
Esophageal atresia (EA) = OA occurs when the esophagus doesn’t attach to the stomach; therefore, food can’t get from the esophagus into the stomach. The main symptoms of EA include vomiting and drooling.
How Are the Problems Diagnosed?
If your baby has problems eating or breathing, chokes during feeding, or coughs up a lot of fluid or mucus, he or she may have TEF or EA. = TOF or OA Your health care provider will take an X-ray to learn more. This will show if the baby has one or both problems. The X-ray is often done with a feeding tube put into the baby’s esophagus to see if the tube reaches the stomach.
How Are the Problems Treated?
Both of these problems require surgery. Your baby will receive nourishment through an IV (intravenous) line until surgery can be done. A breathing machine may also be needed:
To treat TEF = TOF the opening between the trachea and esophagus is closed during surgery.
To treat EA = OA the esophagus is connected to the stomach. In some cases, a tube with a weighted tip is put into the esophagus. This helps stretch the tissues to reach the stomach. It may take a few weeks before the esophagus is long enough to reach the stomach. The baby will stay in the neonatal intensive care unit during this time. When the esophagus is long enough, surgery is done to attach it to the stomach.
What Are the Long-Term Effects?
EA = OA Treatment of TEF = TOF often has a good outcome. Once the fistula is closed, many babies don’t have problems. But in some cases, ongoing breathing problems can occur. can cause more serious problems. If the esophagus must be stretched, your baby may have permanent swallowing problems. Many babies develop GERD (gastroesophageal reflux disease). Also, your baby will have been fed through an IV until after treatment. As a result, your baby may have trouble moving on to breast or bottle feeding. For instance, your baby may have trouble learning how to suckle and breathe at the same time. The doctor can tell you more about how your baby is likely to progress.
EA montage for EA/TEF OA/TOF Awareness Esophageal Oesophageal Atresia
What is Aspiration?
Aspiration in children is a serious and common problem. It usually presents with an initial episode of choking with subsequent respiratory symptoms. Aspiration occurs whenever secretions, solid food or liquids “go down the wrong pipe” and enter the airway and lungs. Aspirating material into the lungs can lead to respiratory problems, such as pneumonia. While there may be observable signs that accompany aspiration events, such as coughing, choking, eye reddening during eating or a gurgly vocal quality after swallowing, infants and children can also aspirate “silently,” or with no observable symptoms.
If your child is found to be aspirating, follow-up therapy is recommended to work with you and your child to develop a feeding/swallowing program based on your child’s unique needs. Signs and risks for aspiration
The ability to swallow safely is the primary prerequisite for becoming an oral feeder. When a child aspirates, oral feedings are often discontinued; and the child is given a feeding tube for eating. Many professionals recommend stopping the use of food at home and in therapy programs until the child swallows without aspirating on a modified barium swallow study. This leaves parents and therapists with many questions and implies a wait-and-see approach.
Aspiration is when something enters the airway or lungs by accident. It may be food, liquid, or some other material. This can cause serious health problems, such as pneumonia. Aspiration can happen when a person has trouble swallowing normally. This is known as dysphagia. It can also happen if a child has gastroesophageal reflux disease (GERD). This is when the contents of the stomach come back up into the throat.
When your child swallows food, it passes from the mouth down into the throat. This is called the pharynx. From there, the food moves down through a long tube (oesophagus) and into the stomach. This journey is made possible by a series of actions from the muscles in these areas. If your child has dysphagia, the muscles don’t work normally. They cause problems with the swallowing process.
The pharynx is also part of the system that brings air into the lungs. When a person breathes, air enters the mouth and moves into the pharynx. The air then goes down into the main airway (trachea) and into the lungs. A flap of tissue called the epiglottis sits over the top of the trachea. This flap blocks food and drinks from going down into the trachea when your child swallows. But in some cases, food or drink can enter the trachea. It may go down as your child swallows. Or it may come back up from the stomach. A child with dysphagia is much more likely to aspirate. A child with a developmental or health problem is more likely to have dysphagia.
Aspiration can happen during a feeding or meal. And it can happen after a feeding or meal. This is common for babies and children with certain health conditions. Aspiration can also happen when at any time when your child swallows saliva.
If your child aspirates a small amount of material, it may not cause much harm. This can happen in children who don’t have a health problem. It can happen when eating, sleeping, or talking. But aspiration that happens often or in a large amount can be serious.
This Page is to try and give you an insight of having a child born unable to swallow.
What are Stickies? in my day it was known as Chocking on Food Stuck. Here are some Parents Coments on how they cope with their Child, taken from our Group linked to this Website
With what you read below here are how other Parents cope with food getting stuck. My advice is this, try not to panic in front of your child, you only make it worse for the child, I always say this to Parents I meet. ( If you’re born with two legs and you have one removed, later on, you know you should have two ) BUT if born with the one you learn to cope.
So you’re Child is born unable to swallow he or she knows nothing else, so will learn to cope as they grow, I did, I learned how I could remove food I had my own way of dealing with it, trust me it did not always work so then it was a trip into the local Hospital, whereas a child I spent a hell of a lot of time, but we are talking 1960 to 1980.
You will grow to understand you’re child’s needs better than any Doctor, this road will not be easy at times but you are not on your own, WE ARE HERE Parents and Adults who have been through what you are going to as well.
Parents Comments on how they deal with food getting stuck now known as STICKIES.
We use coke and lemonade if food gets stuck the fizz either wash it down or fizzes it up plus back slaps or rocking on the knee all work wonders for us xxx
We hang our 2-year-old upside down and pat her back. 99% of the time she gags it up on her own. I’ve had to put my finger down her throat a couple of times to make her vomit.. and only one time she had an endoscopy.
Granddaughter is older now and is better at eating, drinking lots of water, however just in case, my daughter & son-in-law keep Minnie Sprite cans around as a last resort.
Prior to eating, I give my son very warm ( not hot enough to burn him) tea or water with lemon. I feel that the warmth relaxes the esophagus and he eats well and nothing has ever been stuck.
I always try the thump on the back. If that doesn’t work it’s a drink of coke or pineapple juice. But every time Sharon eats she has a drink of water beside her.
My dad used to hang me upside down as a child and smack my back.
We used to try yogurt to help it slip down
Full fat coke
Pineapple juice
All of those and a little time
If no movement after an hour we would go in
If breathing was compromised we would ring ambulance without question
I put my baby over my knee and give her a tap on the back or big drink of water.
Bouncing her up and down while banging her back or over my knee and back taps when she was younger. Now she’s 4 we put her on the trampoline to bounce or coke, yogurt or pineapple juice help.
When Kes was little, I had to resort to thumping her on the back (occasionally hard). These days (she’s now 14), she pushes with some force on the soft skin at the base of her throat while taking a big mouthful of water and swallowing hard.
Water first then fizzy pop if still stuck then thump her back over my knee.
I had to put my finger in my baby mouth to get food out, it was a most horrible experience I had with him, believe it or not, I am so scared of feeding him solid food,
It’s terrifying ladies, my daughter is now 2 and every day seems to get easier. She seems to now understand that if she doesn’t chew enough, it’ll hurt to swallow or get stuck.
When mine was a baby… Over my knee on her tummy and thump on her back…. When she was older thump her back hard. And coke… Coke always worked… I looked like a bad mum feeding her ‘junk’ food lol
Back in the 1970s before any kind of support and even before Dilatations were a ‘thing’. My dad would whisk me outside tip me upside down and encourage me to vomit! That was IT the only solution for my whole childhood. True for us pioneer oldies.
If Kaleb cannot cough it up…..we stick our finger down his throat to make up throw up. It is not very often we have to do this as we WATCH his intake – feed him like a little baby bear! :) With that said….No fancy manicured fingernails for this mommy or I (gramma) The things you do…Right ?? Who would have thought…….
I tap my sons back and then I give him chest thrusts if that doesn’t help I put my finger into his mouth to make him vomit.
My kiddo 16-months tef ea type c gags till it comes out.
THIS WILL GET EASIER as you learn how works better for you x
A device called EndoFLIP — offers a more complete view of digestive disease than existing diagnostic procedures.
A Better View of Esophagus Dysfunction
A technology known as EndoFLIP® (endoluminal functional lumen imaging probe) is a newer, minimally invasive device created to complement traditional diagnostic tests, such as high-resolution esophageal manometry and barium esophagram.
Both of the traditional diagnostic tests are useful in most cases. The esophagram visually demonstrates the clearance of the bolus — swallowed material — from the esophagus. And while manometry measures the strength of contraction in the esophagus, the probe is very thin and may not accurately represent the mechanics of the esophagus in response to a bolus of food.
EndoFLIP uses a balloon mounted on a thin catheter placed transorally at the time of a sedated endoscopy. In comparison to the traditional diagnostic tests, EndoFLIP offers the additional capability of measuring the cross-sectional area and intraluminal pressure of the esophagus while under distension (as if a solid bolus was present). The technology uses impedance planimetry to estimate the cross-sectional area.
The University of Michigan Esophageal Disorders Program is one of a handful of centers in the region with experts trained to use this EndoFLIP technology. (At the time of writing this)
Barium Swallow
This is an examination that evaluates your esophagus. The esophagus is the muscular tube that connects your mouth to your stomach. The study will involve drinking a barium mixture which can be seen with x-rays. You may be given some crystals to swallow, which produce gas in your stomach and esophagus. A series of x-ray images will be taken.
Esophageal Manometry
High-Resolution Esophageal Manometry (Esophageal Mano) Esophageal manometry examines the movement and pressures of your esophagus, how is Esophageal Manometry Performed?
This test will involve the placement of a small catheter through your nasal passage, or nostril, and then swallowed into your esophagus with drinks of water. The catheter is a bit thicker than the power cord for a smartphone. You will be able to swallow, talk, and breathe without any difficulty during the test. We will record the movement and pressures of your esophagus as you drink small amounts of water. Your appointment will take about 1 hour. The tube will be in your nose and down your esophagus for 15 to 20 minutes. You should not eat or drink after midnight the night before your test when scheduled for a morning appointment. If scheduled for an afternoon appointment, you may have clear liquids until 9 a.m. on the day of your exam, then nothing by mouth after that time. Your doctor might additionally recommend fasting except for clear liquids at least 24 hours before the procedure You can take most of your typical morning medications with small sips of water.
How the EndoFLIP works
During an upper endoscopy (EGD), a catheter is passed transorally into the stomach. A balloon attached to the catheter is inflated with a specific concentration of a solution with known ionic properties to various volumes.
A small electrical current is passed through an electrode located on the catheter inside the balloon. The current can only pass to its paired electrode through the solution in the balloon. The voltage gradient between the pair of electrodes is inversely proportional to the cross-sectional area at the midpoint between the pair of electrodes.
The catheter has multiple pairs of electrodes along its length which are sequentially activated.
Simultaneously, the pressure in the balloon is measured. The software calculates the distensibility index (the ratio of the cross-sectional area to the pressure). Data is manually reviewed after the procedure.
How it feels
From the patient’s perspective, a diagnostic EndoFLIP procedure feels just like an EGD. EndoFLIP can also be used therapeutically to provide pneumatic dilation for achalasia — a specific condition where the lower esophageal sphincter fails to relax to permit passage of the bolus, causing difficulty swallowing — without using the traditional method, which necessitates radiation exposure by fluoroscopy.
The EndoFLIP is particularly helpful in cases where the findings on manometry and esophagram are discordant for an achalasia diagnosis. It may also be helpful in achalasia patients who have a recurrence after treatment — EndoFLIP is useful in determining whether a repeat procedure directed at the lower esophageal sphincter would be beneficial for the patient or not.
The idea was presented at Digestive Diseases Week 2015 on what thresholds of distensibility of the esophagogastric junction should be used for diagnosing achalasia.
Importantly, we found that the distensibility of the esophagogastric junction in patients following successful fundoplication for GERD is similar to that in patients with achalasia. This means that the distensibility of the esophagogastric junction needs to be interpreted in the context of the demonstrated motility of the body of the esophagus. This highlights the clinical pearl that patients being considered for fundoplication for regurgitation symptoms should routinely undergo esophageal manometry pre-operatively to exclude peristalsis in the body of the esophagus, as such patients would be at high risk for dysphagia following fundoplication.
In the future, we hope that EndoFLIP may be able to distinguish phenotypes of achalasia or other dysmotility that can help guide specific management.
For now, we Doctors continue to use EndoFLIP as a diagnostic tool and to deliver pneumatic dilation without the need for exposing the patient to fluoroscopy.
How far the Surgeons have come filmed in 2019 Robotic placement of LINX device utilizing EndoFLIP for sizing (Age-restricted video (based on Community Guidelines)
Responsive website designed & developed by
We use cookies to help improve your experience of this website. By using this website, you agree to accept cookies from this site.